Free Printable Health Care Surrogate Form
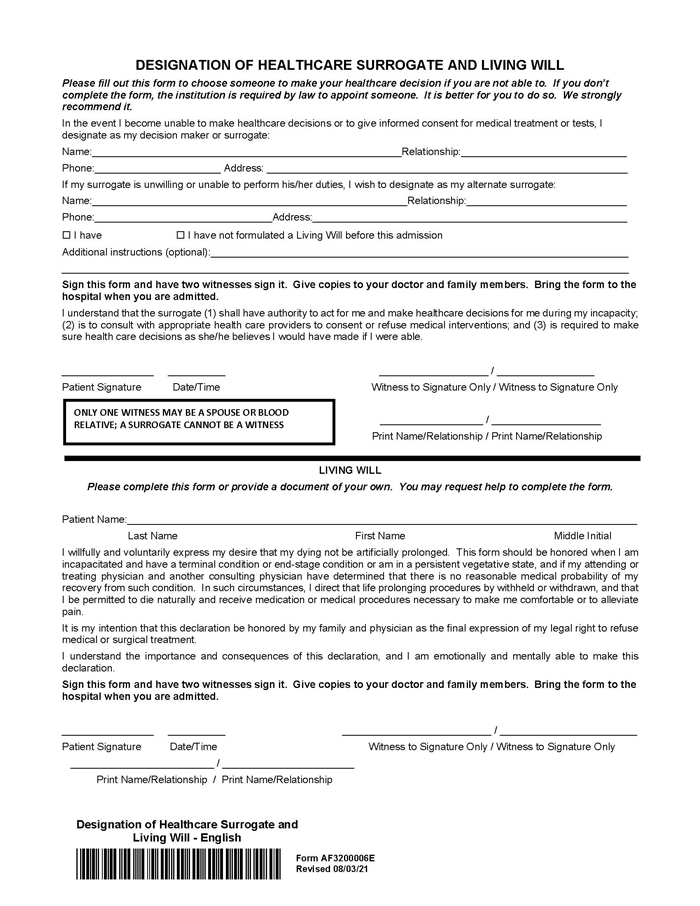
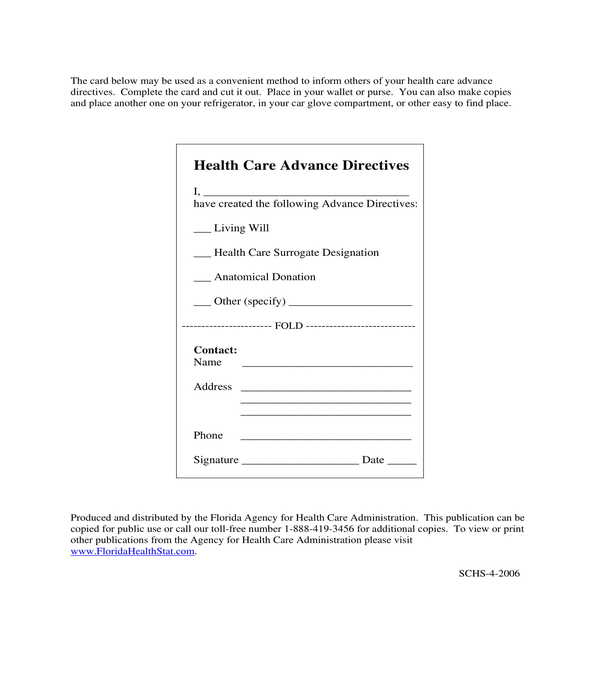
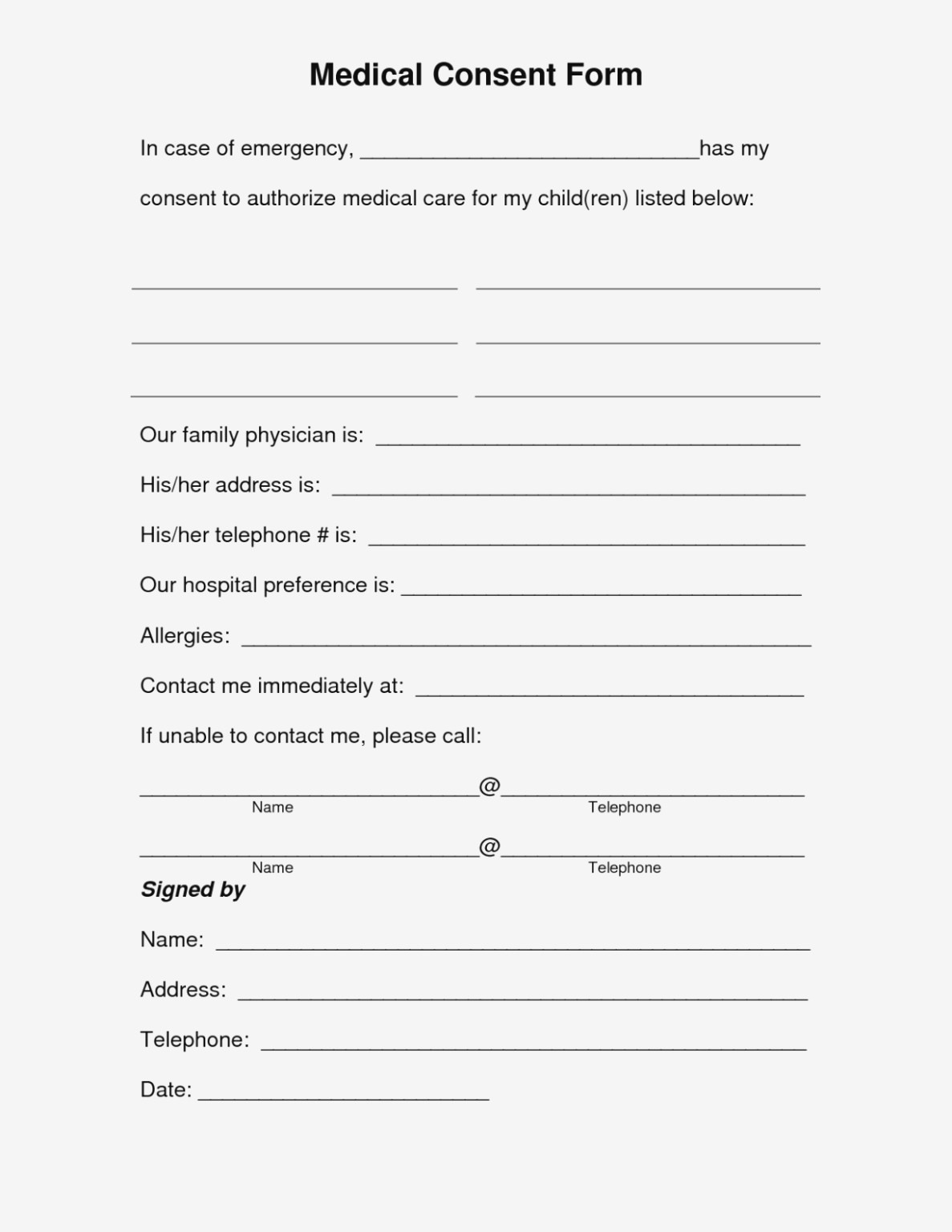
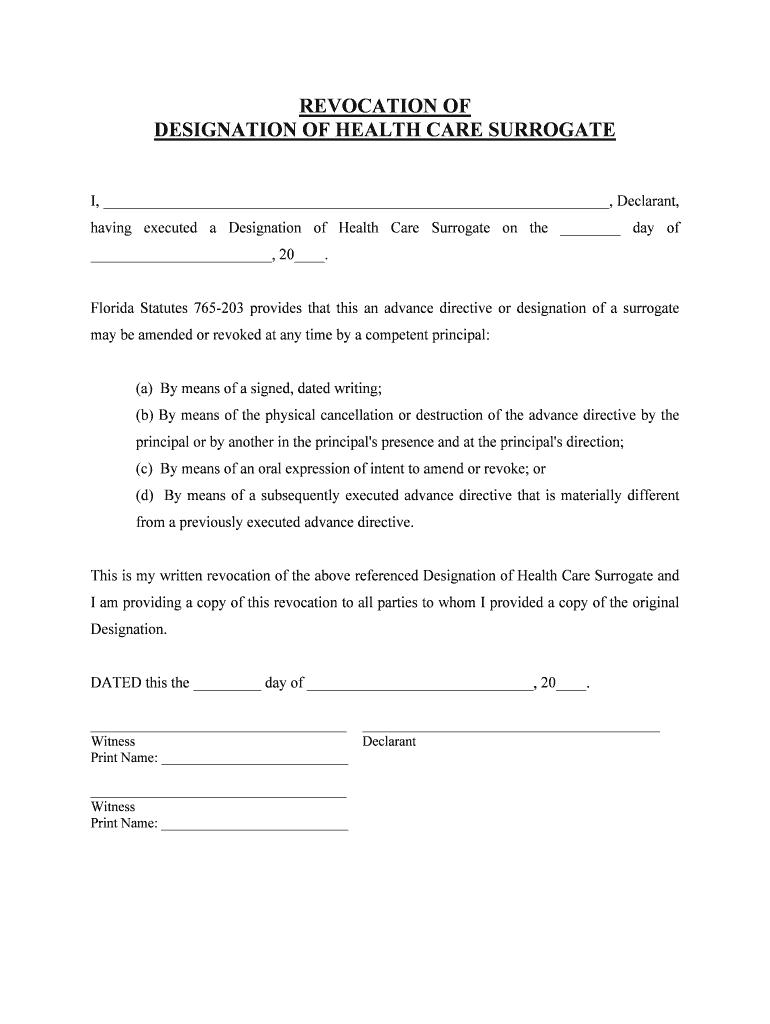
Free Printable Health Care Surrogate Form - Web request a free printed or digital version of our advance directive guide. Web instructions for my health care surrogate: Please fill out this form to choose someone to make your healthcare decision if you are not able to. A health care surrogate form is a type of advanced health care directive document which is used by doctors and healthcare agencies for their patients who may have the possibility to be incapacitated due to their medical conditions. It is best to use your given name; If i initial this box ______________, my health care surrogate’s. To apply for public benefits to defray the cost of health care; Web all competent adults, 18 years of age or older, can appoint a health care agent by signing a form called a health care proxy. Web if my surrogate is unwilling or unable to perform his or her duties, i wish to designate the following person[s] as my surrogate[s] to make health care decisions for me as authorized by this document*[, and they shall serve in the following order]*: Web • a health care surrogate designation • an anatomical donation you might choose to complete one, two, or all three of these forms. Web designation of health care surrogate. To apply for public benefits to defray the cost of health care; Web instructions for my health care surrogate: A florida medical power of attorney, or ‘florida designation of health care surrogate’ or ‘advance directive’, allows a person to appoint a surrogate and an alternate surrogate to make health care judgments if. It is best to use your given name; Authorize my treatment or have treatment stopped based on my choices and values. Web • a health care surrogate designation • an anatomical donation you might choose to complete one, two, or all three of these forms. If i am unable to express my wishes or make my medical decisions, my health care surrogate (hcs) will: It is a written or oral statement of the kind of medical care you want or do not This pamphlet provides information to help you decide what will best serve your needs. Apply on my behalf for private, public, government, or veterans’ benefits to defray the cost of health care. Apply on my behalf for private, public, government, or veteran’s benefits to defray the cost of health care. Instructions for my health care surrogate: Web • a health care surrogate designation • an anatomical donation you might choose to complete one, two, or all three of these forms. Web if my surrogate is unwilling or unable to perform his or her duties, i wish to designate the following person[s] as my surrogate[s] to make health care decisions for me as authorized by this document*[, and they shall serve in the following order]*: It is best to use your given name; And to authorize my admission to or from a health care facility. A living will and a designation of health care surrogate form, which is sometimes known as a durable power of attorney for health care or medical power of attorney. When would my health care agent begin to. It is a written or oral statement of the kind of medical care you want or do not If you don’t complete the form, the institution i s required by law to. Apply on my behalf for private, public, government, or veteran’s benefits to defray the cost of health care. I, (name) my health care team. , want to choose how i will be treated by. Web i fully understand that this designation will permit my designee to. Talk to my health care team and have access to my medical information. Web find advance directives forms by state. , want to choose how i will be treated by. It is a written or oral statement of the kind of medical care you want or do not En español | when planning for your future medical care, prepare your. Web • a health care surrogate designation • an anatomical donation you might choose to complete one, two, or all three of these forms. Web health care surrogate designation documents are readily accessible for free online, are easy for most people to understand, and (in most cases) can be filled out in the comfort of your own home. It is. Talk to my health care team and have access to my medical information. Talk to my health care team and have access to my medical. Fill in your full name on the first line. I, (name) my health care team. It is best to use your given name; To apply for public benefits to defray the cost of health care; If i am unable to express my wishes or make my medical decisions, my health care surrogate (hcs) will: If i initial this box ______________, my health care surrogate’s. Apply on my behalf for private, public, government, or veteran’s benefits to defray the cost of health care. If. Web the purpose of this document is to direct the provision, the withholding or withdrawal of life prolonging procedures in the event one should have a terminal condition. A health care surrogate form is a type of advanced health care directive document which is used by doctors and healthcare agencies for their patients who may have the possibility to be. If you don’t complete the form, the institution i s required by law to. If i initial this box ______________, my health care surrogate’s. Lets you choose another person to make medical decisions based on your wishes for medical treatment, if you are not able to make your own decisions or if you choose not to make them for yourself.. Apply on my behalf for private, public, government, or veterans’ benefits to defray the cost of health care. Web in the event that i have been determined to be incapacitated to provide informed consent for medical treatment and surgical and diagnostic procedures, i wish to designate as my surrogate for health care decisions: Please fill out this form to choose. Both can be changed anytime, and you’ll want to update them periodically. If i am unable to communicate or make my medical decisions, my health care surrogate (hcs) will: When would my health care agent begin to. This pamphlet provides information to help you decide what will best serve your needs. It is best to use your given name; Apply on my behalf for private, public, government, or veteran’s benefits to defray the cost of health care. A health care surrogate form is a type of advanced health care directive document which is used by doctors and healthcare agencies for their patients who may have the possibility to be incapacitated due to their medical conditions. Please fill out this. A living will and a designation of health care surrogate form, which is sometimes known as a durable power of attorney for health care or medical power of attorney. Fill in your full name on the first line. Lets you choose another person to make medical decisions based on your wishes for medical treatment, if you are not able to make your own decisions or if you choose not to make them for yourself. Web i fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; Web find advance directives forms by state. This pamphlet provides information to help you decide what will best serve your needs. I, (name) my health care team. You don’t need a lawyer or a notary, just two adult witnesses. Web in the event that i have been determined to be incapacitated to provide informed consent for medical treatment and surgical and diagnostic procedures, i wish to designate as my surrogate for health care decisions: If you don’t complete the form, the institution i s required by law to. The form will automatically add your name in every location. Apply on my behalf for private, public, government, or veterans’ benefits to defray the cost of health care. A florida medical power of attorney, or ‘florida designation of health care surrogate’ or ‘advance directive’, allows a person to appoint a surrogate and an alternate surrogate to make health care judgments if. Apply on my behalf for private, public, government, or veterans’ benefits to defray the cost of health care. Apply on my behalf for private, public, government, or veteran’s benefits to defray the cost of health care. Web there are two different types of advance directives: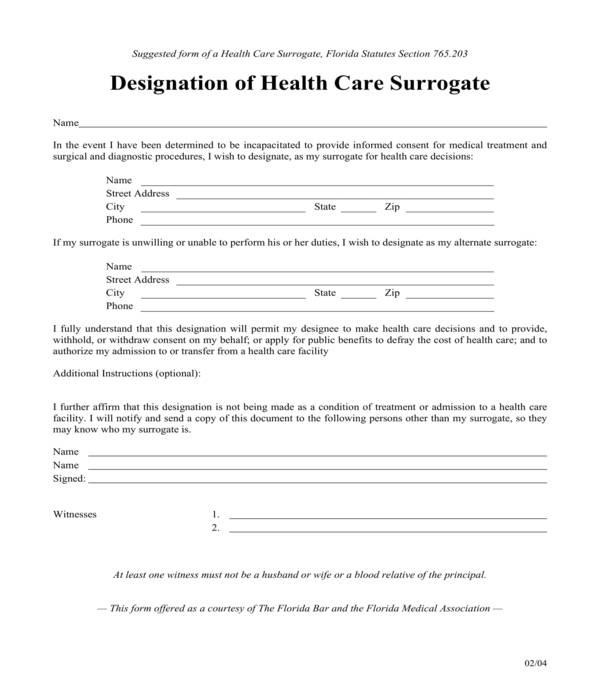
FREE 5+ Health Care Surrogate Forms in PDF
Designation of Healthcare Surrogate and Living Will Sylvester

Health Care Surrogate Worksheet —
Healthcare Surrogate Form Fill Out, Sign Online and Download PDF

Health Care Surrogate Form Family Health
FREE 5+ Health Care Surrogate Forms in PDF
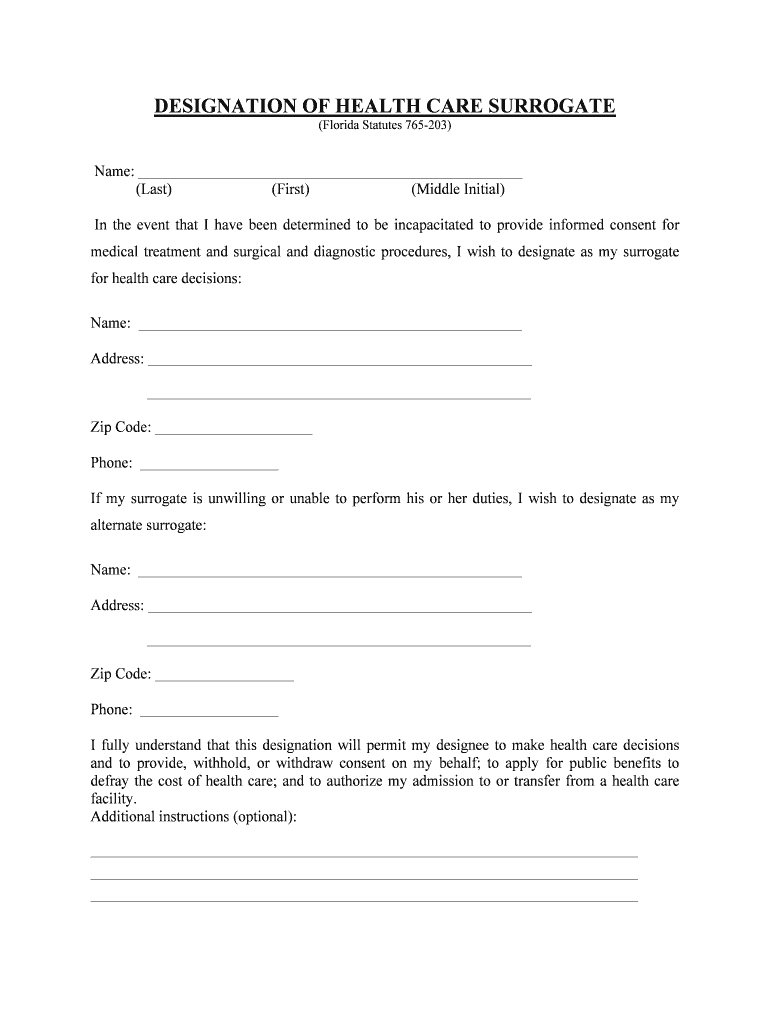
Health Care Surrogate Form Florida Fill Online, Printable, Fillable
Health Care Surrogate Form Florida Universal Network —
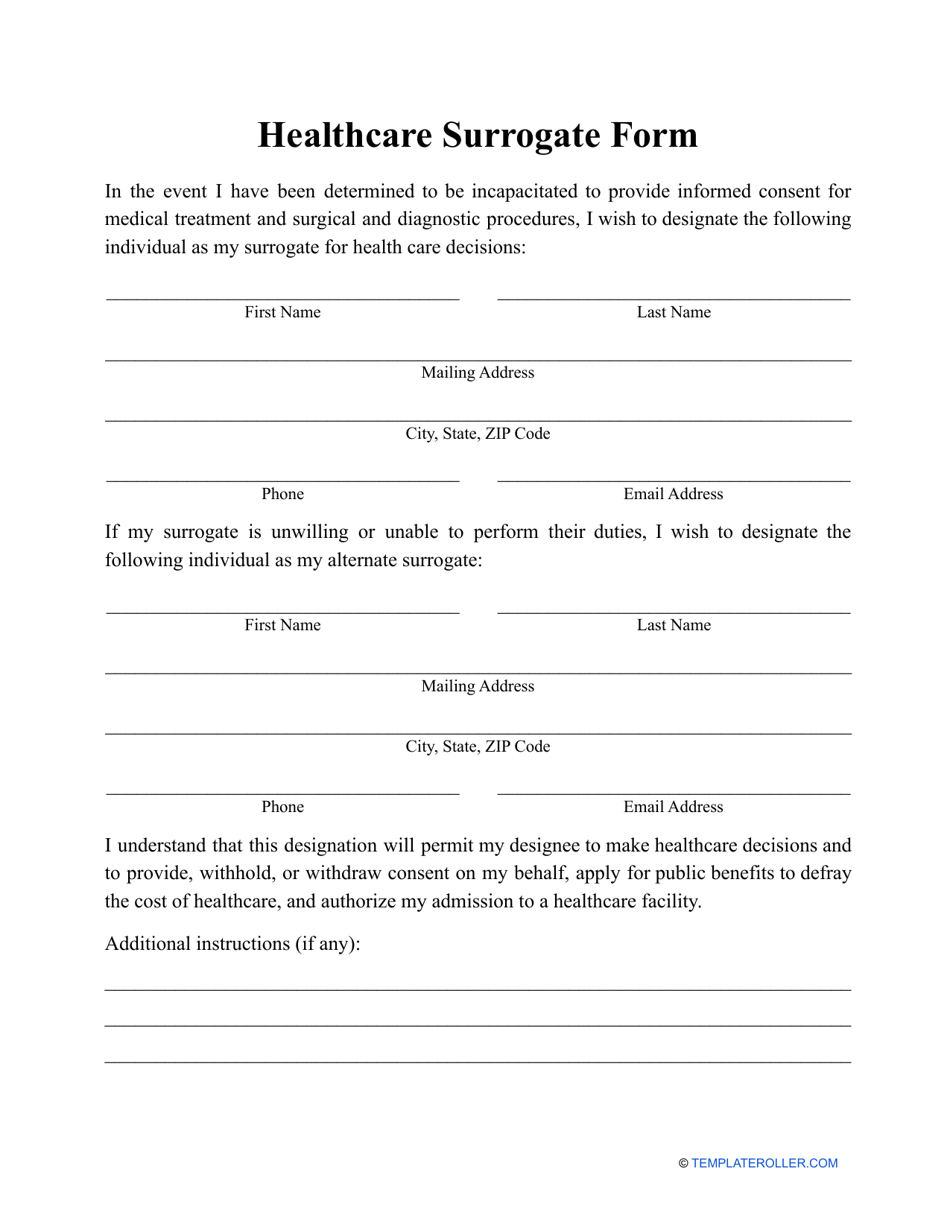
Healthcare Surrogate Form Fill Out, Sign Online and Download PDF
Designation of a Health Care Surrogate Statutes Form Fill Out and
, Want To Choose How I Will Be Treated By.
The Suggested Form Of This Instrument Has Been Provided By The.
Authorize My Treatment Or Have Treatment Stopped Based On My Choices And Values.
If I Initial This Box ______________, My Health Care Surrogate’s.
Related Post: