Printable Medical Clearance Form For Dental Treatment
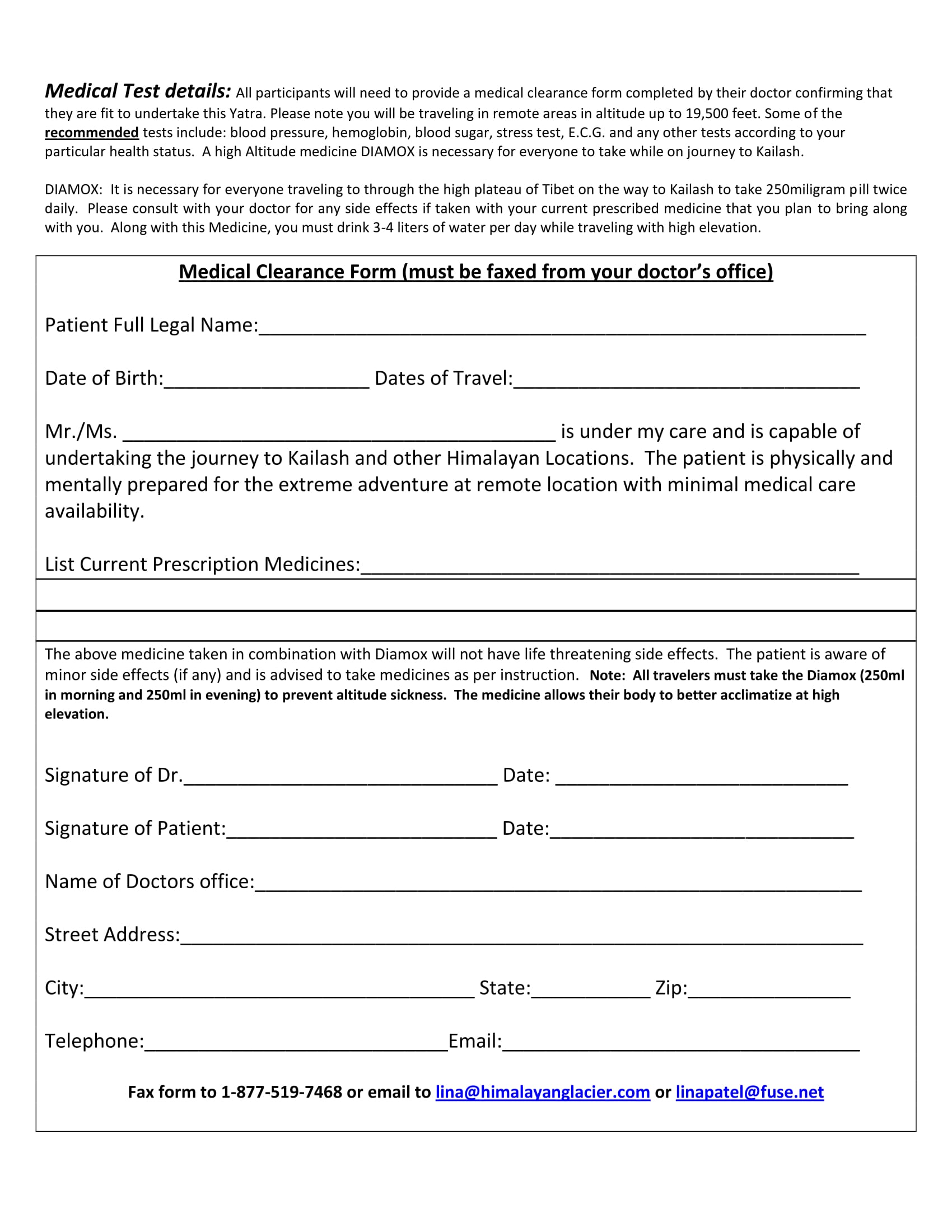
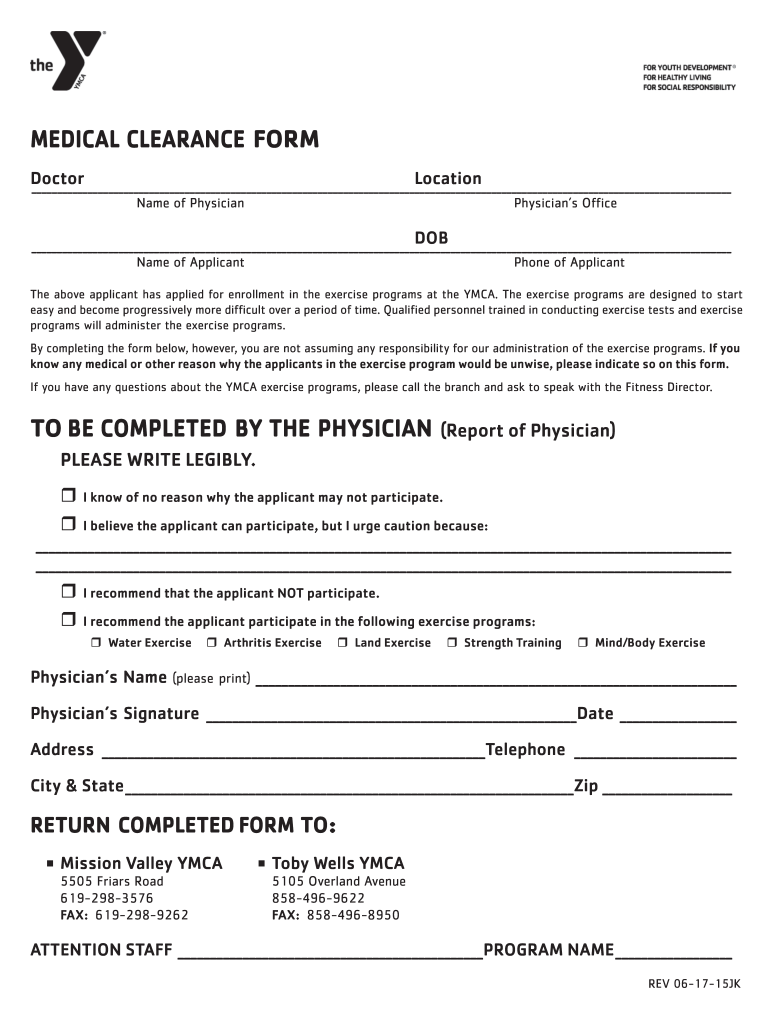
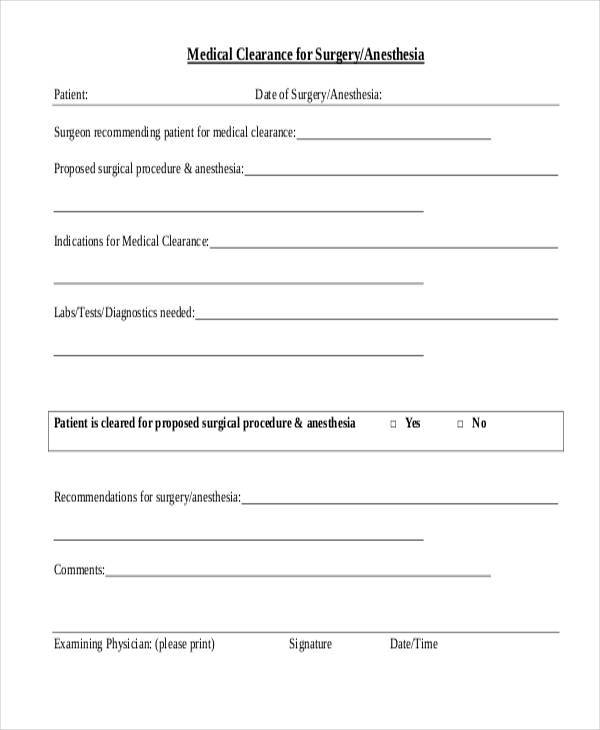
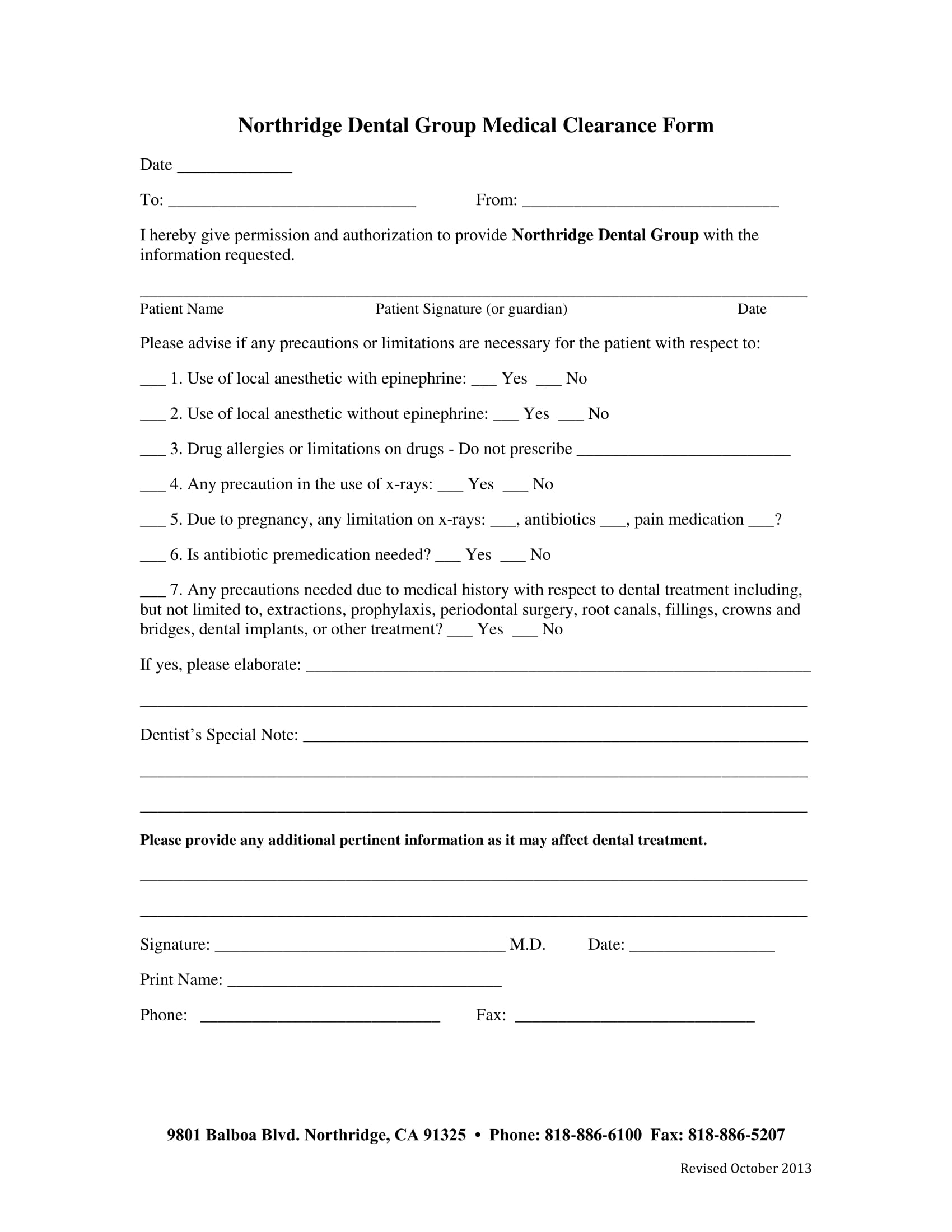
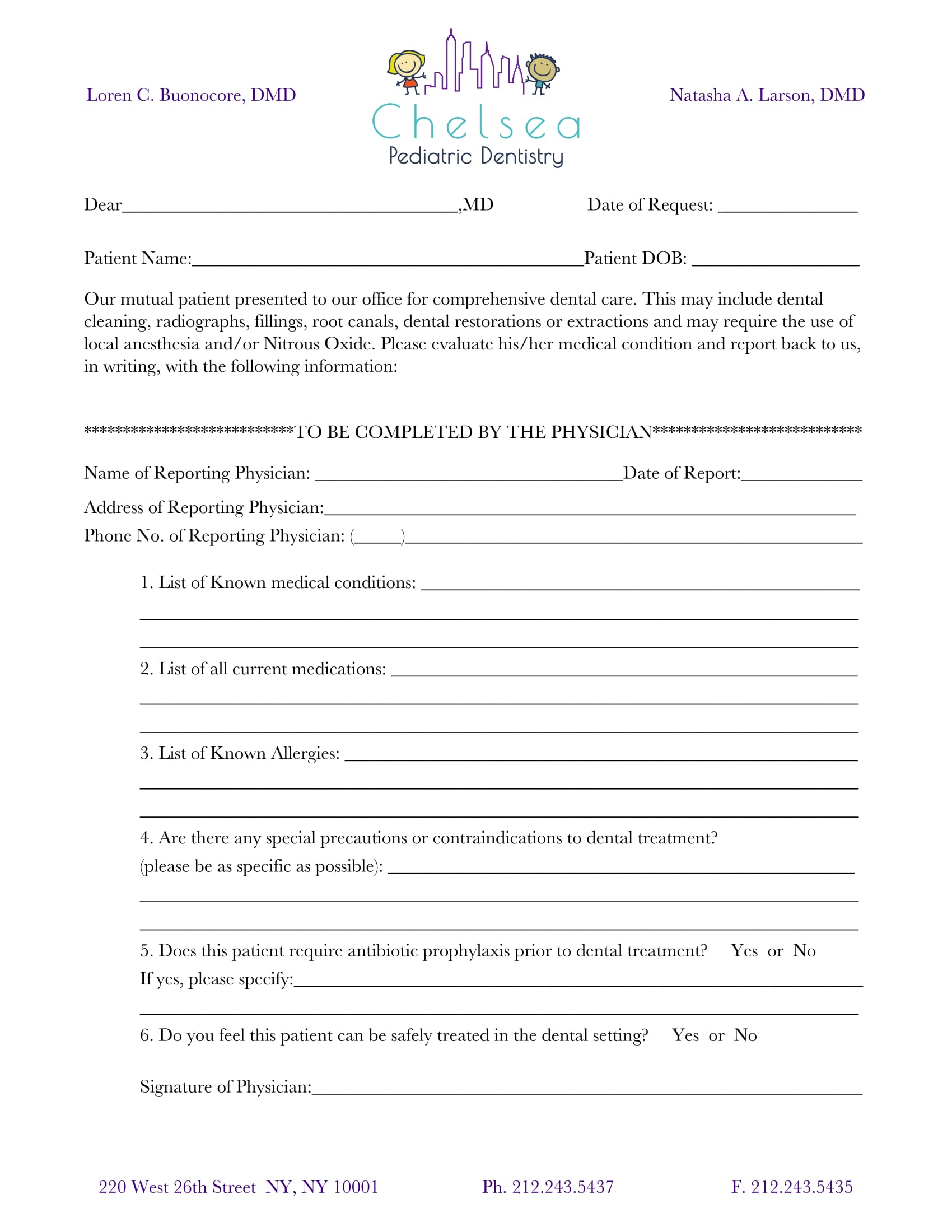
Printable Medical Clearance Form For Dental Treatment - Web our mutual patient, as noted above, is scheduled for dental treatment at our office. Web if you’re a dental office manager, use a free dental clearance form template to collect patient information online! Web medical clearance form (confidential) instructions: Web dear dental provider, our mutual patient is in need of dental treatment. Ensure a smooth journey to treatment. Web a dental medical clearance form is a document requested by dental professionals prior to performing certain dental procedures that could potentially impact a patient's overall health, especially if they have underlying conditions like coronary artery disease. Cleaning (simple or deep) radiographs with appropriate abdominal shielding. Web medical clearance form for dental treatment. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: You can also download it, export it or print it out. Ensure a smooth journey to treatment. Web the patient has indicated the following medical conditions: To proceed with dental treatment, this form is required from a medical physician. Cleaning (simple or deep) radiographs with appropriate abdominal shielding. Web cocodoc is the best platform for you to go, offering you a great and easy to edit version of medical clearance form for dental as you require. This medical clearance form requests information from a patient's primary physician to approve dental treatment. The patient has indicated the following medical conditions: Web dear dental provider, our mutual patient is in need of dental treatment. Please complete the section below. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Web our mutual patient, as noted above, is scheduled for dental treatment at our office. Please complete this form entirely so that we can safely render the best possible dental care for our mutual patient. Web medical clearance for dental treatment. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Ensure a smooth journey to treatment. Just customize the form to match your dental office’s look and feel — then embed it in your website, share it with a link, or print it out to collect with a tablet or computer. Web edit, sign, and share printable medical clearance form for dental treatment online. Section 1 to be completed by the dentist 1. You can also download it, export it or print it out. Dentist name (please print) dentist signature date physicians: Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Ensure a smooth journey to treatment. No need to install software, just go to dochub, and sign up instantly and for free. This medical clearance form requests information from a patient's primary physician to approve. Cleaning (simple or deep) root canal therapy. The patient has indicated the following medical conditions: Its complete collection of forms can save your time and jumpstart your efficiency massively. Web if you’re a dental office manager, use a free dental clearance form template to collect patient information online! Web the patient has indicated the following medical conditions: Web the patient has indicated the following medical conditions: Please complete this form entirely so that we can safely render the best possible dental care for our mutual patient. Type text, add images, blackout confidential details, add comments, highlights and more. Please complete the section below. Our mutual patient has presented for dental treatment with the following medical problem(s): Edit your printable medical clearance form for dental treatment online. Ensure a smooth journey to treatment. Section 1 to be completed by the dentist 1. Web medical clearance form (confidential) instructions: Web medical clearance form for dental treatment. £ cleaning (simple or deep) £ root canal therapy £ radiographs £ fillings, crowns, bridges £ extractions (simple or surgical) £ nitrous oxide £ local anesthetic (with epinephrine) £ other: Web our mutual patient, as noted above, is scheduled for dental treatment at our office. Ensure a smooth journey to treatment. Web this article presents recommendations related to patients with. Web the patient has indicated the following medical conditions: Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Web in surgery, a medical clearance form can help determine if a proposed course of treatment will adversely affect the patient’s condition or if the patient’s. Web streamline your medical treatment process with our comprehensive dental clearance form. Does the patient require antibiotic prophylaxis? Use of local anesthesia to control pain failed or was not feasible based on the medical needs of the patient. Please evaluate this patient’s medical history and advise us of any special considerations that should be made. Web send medical clearance for. Cleaning (simple or deep) radiographs with appropriate abdominal shielding. Use of conscious sedation, either inhalation or oral, failed or was not feasible based on the medical needs of the patient. Web our mutual patient is scheduled for dental treatment. Web in order for us to deliver safe and efficient dental treatment while being aware of patient’s medical condition, i would. Web send medical clearance for dental treatment via email, link, or fax. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Use of conscious sedation, either inhalation or oral, failed or was not feasible based on the medical needs of the patient. Web in. Its complete collection of forms can save your time and jumpstart your efficiency massively. Web our mutual patient is scheduled for dental treatment. Dentist name (please print) dentist signature date physicians: Web send medical clearance for dental treatment via email, link, or fax. No need to install software, just go to dochub, and sign up instantly and for free. Please evaluate this patient’s medical history and advise us of any special considerations that should be made. Web medical clearance form for dental treatment. Web dental provider, please check at least one of the below reasons for general anesthesia: Web the patient has indicated the following medical conditions: Use of conscious sedation, either inhalation or oral, failed or was not feasible based on the medical needs of the patient. Cleaning (simple or deep) radiographs with appropriate abdominal shielding. Web our mutual patient, as noted above, is scheduled for dental treatment at our office. Treatment may include (any exclusions will be lined through): Its complete collection of forms can save your time and jumpstart your efficiency massively. Web streamline your medical treatment process with our comprehensive dental clearance form. This medical clearance form requests information from a patient's primary physician to approve dental treatment. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: Web our mutual patient is scheduled for dental treatment. Does the patient require antibiotic prophylaxis? Use of local anesthesia to control pain failed or was not feasible based on the medical needs of the patient. Section 1 to be completed by the dentist 1.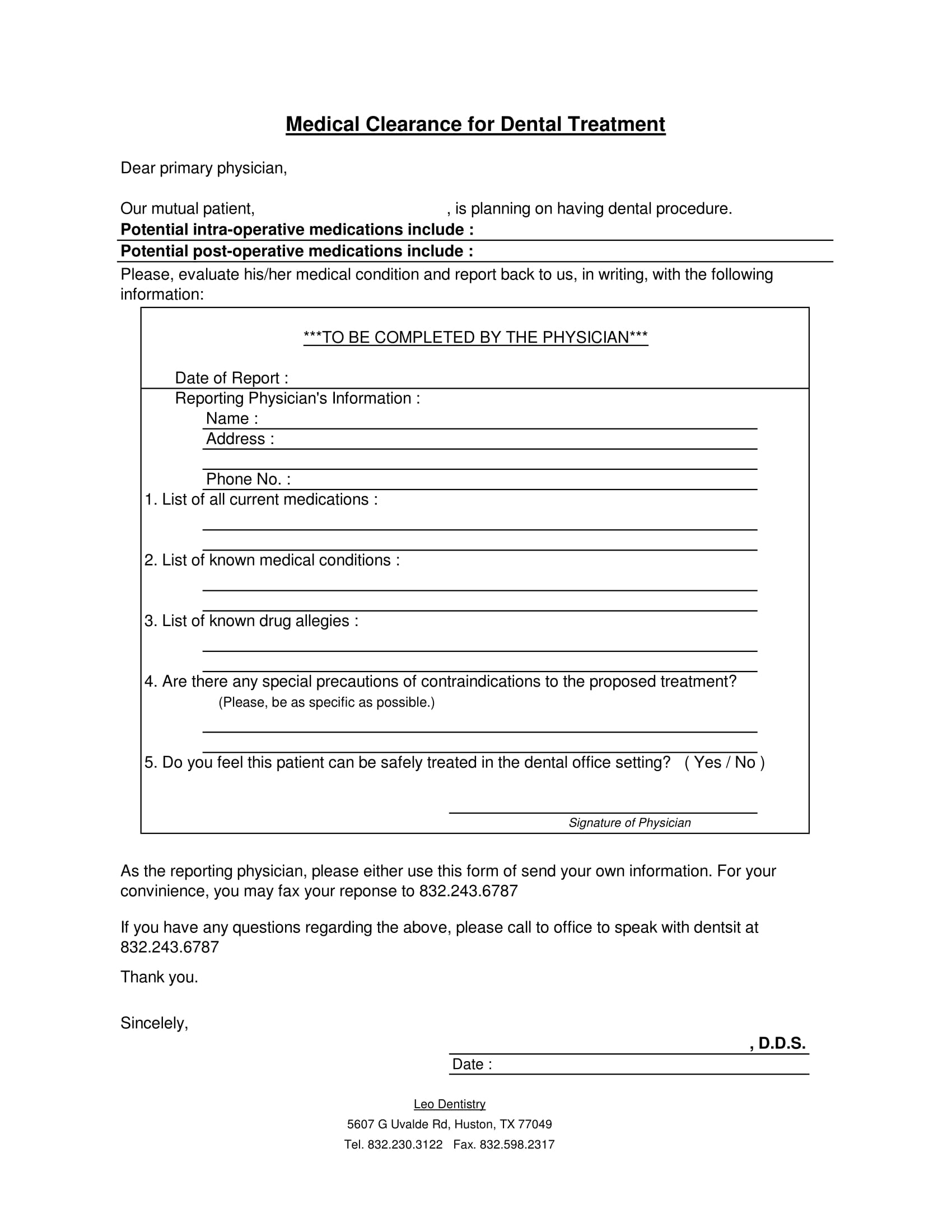
FREE 30+ Medical Clearance Forms in PDF MS Word

Printable Medical Clearance Form For Dental Treatment DocTemplates
Printable Dental Medical Clearance Form
Printable medical clearance form for dental treatment Fill out & sign

Printable Dental Medical Clearance Form
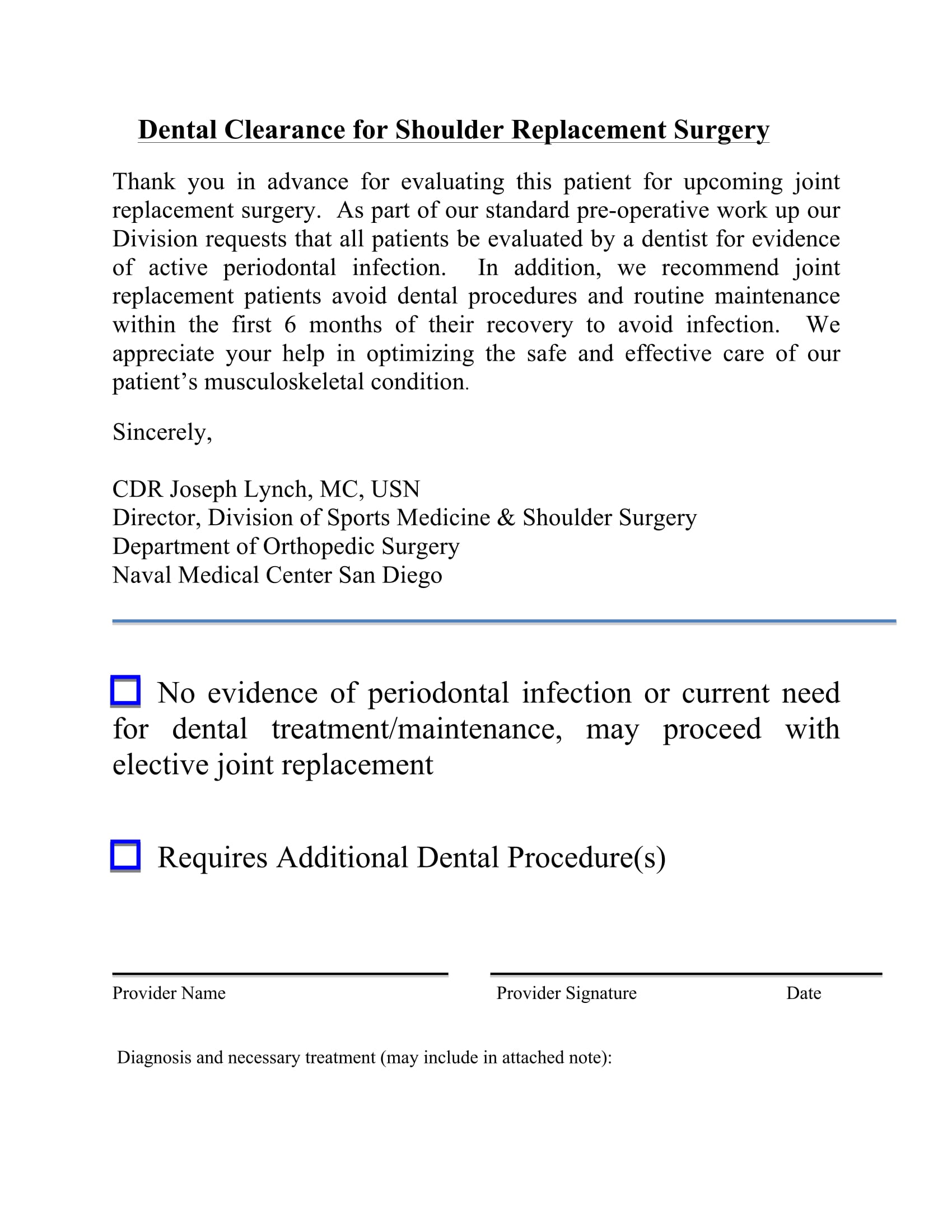
Printable Dental Clearance Form For Surgery Printable Templates
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Type Text, Add Images, Blackout Confidential Details, Add Comments, Highlights And More.
Just Customize The Form To Match Your Dental Office’s Look And Feel — Then Embed It In Your Website, Share It With A Link, Or Print It Out To Collect With A Tablet Or Computer.
Web Dear Dental Provider, Our Mutual Patient Is In Need Of Dental Treatment.
The Patient Has Indicated The Following Medical Conditions:
Related Post: